Cancer will only be beaten when the genomic drivers of a person’s cancer are understood and targeted, according to Brian Tomlinson of Foundation Medicine
Tell me about yourself and your organization
Brian Tomlinson – Medicine Foundation
Foundation Medicine is a molecular information company dedicated to transforming cancer care through a deep understanding of the genomic changes that contribute to each patient’s unique cancer. The company offers a full suite of comprehensive genomic profiling assays to identify the molecular alterations in a patient’s cancer and match them with relevant targeted therapies, immunotherapies and clinical trials.
I joined Foundation Medicine after working for two national cancer patient advocacy Organizations for nearly 18 years. In my role at Foundation Medicine, I lead our external engagement efforts with our patient advocacy partners in the US.
What does personalized medicine mean to you?
Personalized medicine involves providing treatment based on the unique drivers of disease at a molecular level. In cancer, this starts with comprehensive genomic testing to understand what’s driving a patient’s cancer at a molecular level. This gives oncologists and patients the information they need to make informed treatment decisions.
We’re at a critical moment for precision medicine in cancer care. To me, it means finding the right treatment, for the right patient and the right time.
Why do you believe this topic is important?
I am motivated every day by the patients we serve now and the opportunity we have to impact cancer care in the future. Unfortunately, many patients right now do not have access to genomic testing. We have an opportunity to extend lives or even manage cancer as a chronic condition for certain patients today using these breakthrough therapies, but we can only do this when physicians understand the genomic drivers of a patients’ cancer.
As part of our efforts to expand access to genomic testing, we engage with advocacy groups and patients across indications to share scientific insights and serve as a resource on CGP with the goal of expanding overall education and awareness. I have dedicated my career to supporting cancer patients and their families. Having comprehensive testing provides access to really important information about treatment planning and shared decision making.
Why is your organization interested in participating in this multi-stakeholder collaboration? What has your organization been doing in this space?
We believe that transforming cancer care and ensuring all patients can benefit from precision medicine cannot be done alone, which is why we believe collaboration across the ecosystem is so critical. Over the past almost 10 years we’ve established deep partnerships with organizations across academia, industry, biopharma and advocacy.
What makes this collaboration unique?
I think the global focus and the comprehensive external stakeholder engagement make this collaboration a first of its kind and quite unique.
What are your ultimate expectations from the project?
We know expanding access to CGP is critical to increasing the number of patients who can benefit from precision medicine. We’re committed to working across the ecosystem to ensure all patients can benefit from the latest science at the time of care and that oncologists have the tools to make informed treatment decisions. We’re at a true turning point for precision medicine in many regions – including Europe. The healthcare ecosystem has made incredible progress in recent years but there is more work to be done.
Begonya Nafria Escalera of Sant Joan de Déu Children’s Hospital in Barcelona has both a professional and personal interest in ensuring that patients’ needs are met by personalized medicine
Tell me about yourself and your organization
Begonya Nafria Escalera – Sant Joan de Déu Research Foundation
I’m working at Sant Joan de Déu Children’s Hospital as Patient Engagement in Research Coordinator. My area of responsibility is to ensure that the patients and families have an active role, as experts, in any of the research and innovation projects in which our institution is involved. Sant Joan de Déu Children’s Hospital is the largest paediatric hospital in Spain. My background is in social sciences and working in the defence of the patients’ rights for more than 10 years. Also I have a personal story linked with my area of expertise, as I’m caregiver of an adult with cerebral palsy, my brother. In recent years I have also been volunteering with several patient organizations.
What does personalized medicine mean to you?
For me it means the opportunity to offer a treatment for a huge group of complex conditions, the genetic diseases. Most of these conditions affect paediatric patients and there is no cure for them, only in some cases palliative treatments. PM from the patient side means hope but also uncertainty. At this moment, few conditions have the opportunity of these innovative treatments, this means that we need to inform and educate the patients/families about this type of treatment, how it works and what it means to be involved in a clinical trial.
Why do you believe this topic is important?
Because research in new treatments is moving to this direction: try to provide the best and most accurate treatment for the patients. Society and specifically the patients/caregivers need also to move in this direction, knowing what a therapy means, when it works and also the status of research according to the different genetic conditions.
Why is your organization interested in participating in this multi-stakeholder collaboration?
We are increasing our activity in the field of clinical trials in paediatric conditions, as most of these diseases are genetic. For our patients this really can be an opportunity for treatment in the future, considering that probably at the present we don’t have therapeutic options to offer to them. In parallel, in our institution the research model is based on a patient-centric approach, ensuring that in any project in which our institution will be involved patients/families can take part as advisors and/or part of the research team. We have a young person’s advisory group helping in many projects, a board of parents, and according to the needs of every initiative we set up a specific group of patients/parents to help in the design and development of the project. We don’t envision clinical research without the involvement of patients and parents.
What makes this collaboration unique?
For me, it’s the 360 degree approach with a pillar being patient involvement and the issues that need to be addressed to ensure the best quality of life, disease management and empowerment. The activities around health literacy are essential to ensure that any initiative about personalized medicine will be patient-centric, providing patients with the right information to make decisions about their health and treatments.
What are your ultimate expectations from the project?
I am happy to contribute to a global initiative in which patient engagement will be an essential part of the framework, while increasing awareness about health literacy in this field and providing the expertise of working with paediatric patients. As clinical trials in children and young people are global, we need truly collaborative initiatives involving different stakeholders in order to provide the best treatments for the patients, always considering the unmet and specific needs of the most vulnerable groups of patients.
Making personalized healthcare an accessible reality for as many people as possible has been a priority for Sandra Blum of Roche’s Global Patient Partnership team for many years
Tell us more about yourself and your organization.
Sandra Blum – Roche
I am part of the Global Patient Partnership team at Roche. ‘Partnership’ is not just part of our name. It’s a mindset and way of doing things that is highly valued in our organization to develop solutions and medicines that truly meet the needs of individuals, communities and society. Personalized Healthcare is a major focus for Roche and it includes a shift from treating a disease to delivering better care.
What does personalized medicine mean to you?
To me it means that my doctor knows me and my history, and it’s ok if that information comes from a medical record that follows me around wherever I go in the healthcare system or even the world. Together we are able to use all of the available resources to understand my health issues – imaging, diagnostic blood or tissue tests, whatever will give us the best information to work with. Then we discuss and agree on the treatment option(s) that we think will do the most to address my health issues while also taking into account how I like to live my life. And we stay connected to monitor how things are going and make informed decisions about changing course if that’s what we need to do. Plus, all my data will be shared with the right doctor and there is the possibility of improving medical care for others by sharing anonymised data with researchers.
Why do you believe this topic is important?
Health and illness ultimately are very personal, both because of how we experience them but also because we have a growing scientific understanding of how unique diseases are at an individual level. Take cancer as an example. If I get breast cancer, it may be really different than my friend’s breast cancer because of my lifestyle, my body, and the specific ‘fingerprint’ or genetic characteristics of my cancer. In fact, now science is showing us that where a cancer starts – the breast, the colon, the lungs – is only part of the story. That ‘fingerprint’ or genetic make-up of the cancer may ultimately be a better way of understanding what’s driving it and finding the best way to treat it. I’m so passionate about this because it is personal for me, too: my mom died in her 50s of colon cancer. I still miss her pretty much every day. You never know if things could have turned out differently for mom if she had been diagnosed sooner or treated differently. We couldn’t save her but I do hope I can play a role in saving other people, and I think following the science to personalize cancer care, and healthcare in general, is the way forward.
Why is your organization interested in participating in this multi-stakeholder collaboration?
Our vision is to ensure that the screening, diagnosis, treatment and even prevention of diseases will more quickly and effectively transform the lives of people everywhere – ensuring the right treatment for the right patient at the right time.There has been amazing progress in personalizing healthcare over the last 20-plus years, but there is still so much further to go. And not just with research and new advances, but importantly in connecting people to what is available today but may be out of reach in their country or their community. No one can make that kind of change happen alone. We need to work together. FT3 Alliance is an exciting forum to partner with patients, medical experts, companies in biotech/biopharma and other organizations that all share a passion and commitment to making personalized medicine a reality for more people. Roche is so proud to be a FT3 member and collaborator.
What has Roche been doing in this space?
I mentioned that personalized healthcare is abig focus for Roche. We have been really busy working on this for years! Just a few examples… we are bringing together divisions across the Roche group (imaging, diagnostics, pharma) to create integrated solutions that provide personalized healthcare. We have developed digital monitoring tools to make it easier for people to capture and share their health data with their doctors and manage their health. We have a variety of clinical trials looking across cancer types using molecular profiling and targeted treatments as well as capturing real-world data to understand outcomes and inform health system decision-making. Much of what we do is in partnership not only with patients but also with stakeholders in the medical, policy and research communities to collectively create an environment that is ready to deliver personalized healthcare to patients.
What makes this collaboration unique?
FT3 Alliance is a global multi-stakeholder organization focused on personalized healthcare. We have a tremendous opportunity to bring people together from all around the world and from different disciplines to learn about what has been successful and what remains to be done. And because we’re a global network, we can partner with other regional or country-level organizations that are trying to do similar things, so that together we can move faster or do more.
What are your ultimate expectations from the project?
Roche wants to be a part of the change that needs to happen to make personalized healthcare an accessible reality for as many people as possible. Working together, FT3 Alliance has to move quickly beyond analysis, debate and idea generation and into actions that have an impact in countries and communities around the world.
Susan McClure, founder and CEO of Genome Creative, says that while clinical adoption of targeted treatments remains low, multi-stakeholder efforts such as FT3 can change this
Susan McClure – Genome Creative
Tell us more about your organization
We specialize in content strategy, editorial and design updates, event creation and management, websites, podcasts, apps, and marketing. Specifically, we work with partners who share our vision of educating people around how their treatment options are changing thanks to our increased understanding of our DNA. Our goal is to educate people around this exciting time in health care while dispelling myths, explaining the science, and encouraging further exploration.
Genome Creative specializes in creating compelling content that explains complicated topics in a language that everyone can understand. Our team of award-winning science writers and health care journalists are adept at covering this emerging field in a way that is engaging and accessible.
What does personalized medicine mean to you?
I’ve been leading consumer health media companies since 2003, after recovering from an aggressive form of breast cancer. I spent a decade as the publisher of CURE magazine. During my time there, I realized that treatment options were becoming more targeted but clinical adoption and consumer awareness remained low. I am on a mission to fix that.
I left CURE in late 2012 to launch the first national consumer magazine exclusively devoted to genomics. Genome magazine launched in 2014 with the mission of exploring the world of personalized medicine and the genomic revolution that makes it possible, empowering readers to make informed health decisions by improving their health literacy.
While doing research for the business plan, I was truly shocked to see how many treatments that are considered the “standard of care” for conditions like depression, cancer, and Alzheimer’s are ineffective for many patients. Can you imagine if the same standards applied to the auto industry for example? Just imagine how upset you’d be if you paid $70,000 for a car that only ran 25 to 30 percent of the time! We need to demand more of our health care system.
Why is your organization interested in participating in this multi-stakeholder collaboration? What has your organization been doing in this space?
While I am a huge advocate for personalized medicine, I understand the complexities that exist in terms of adoption. I believe that the only way to break down barriers is to bring together a diverse set of stakeholders who are committed to improving access to testing and targeted treatments for any patient who may benefit. My team already works with clients on communication strategies that educate patients about the ways testing and treatment for a variety of conditions are becoming more targeted. We also direct patients to useful resources so they are better equipped to have meaningful conversations with their HCPs about more personalized treatment options.
What makes this collaboration unique?
I believe that this is the first and only global coalition to address this issue by bringing patients, advocates, pharma and diagnostic companies, HCPs, payers, and regulators who will all work together to establish best practices to make personalized care accessible to all people.
What are your ultimate expectations from the project?
My hope is that no matter where a person lives in the world, when faced with a health challenge that could benefit from testing and treatments tailored to the unique characteristics of their disease, they will have easy access to education, information, and support that will enable them to make better health decisions with improved outcomes.
Danielle Barron speaks to FT3 board member Dr. Benedikt Westphalen, Head of Molecular Diagnostics and Therapy Program and the Molecular Tumour Board, Comprehensive Cancer Centre, University Munich, Germany
Dr Benedikt Westphalen is a medical oncologist and molecular biologist, focusing on gastrointestinal oncology and precision oncology. For the last four years, he has been building a precision oncology program at the University of Munich.
Oncology has been transformed in recent years by the concept of personalized medicine. Westphalen explains that, in his field, personalized medicine covers “multiple aspects”.
“The most comprehensive statement would be ‘the right treatment, for the patient at the right time’,” he says. “This covers all aspects from assessing the patient’s prevalence, working with a multidisciplinary team to design and discuss a personalized treatment plan to then realize this plan together with the patient.”
Unsurprisingly, Dr Westphalen is of the belief that personalized medicine should not be a “nice to have”, but rather an essential approach to patient care. In this setting, it is important “to have all necessary tools at hand” to offer patients the most comprehensive oncological care, Westphalen states.
“True personalized medicine, going beyond only focusing on certain aspects in the continuum of oncological care, should be the goal of every practicing oncologist to achieve the best outcome for every individual patient,” he states.
As a healthcare professional and research scientist, Westphalen practices personalized medicine every day. But he believes that the multi-stakeholder collaboration involved in the FT3 project will bring it to the next level.
“FT3 covers an important aspect in personalized medicine, namely the interplay between comprehensive biomarker testing and treatment decisions based on the individual profile of a patient’s tumor. Modern oncology increasingly depends on this interplay.”
Yet, there are still many roadblocks in place, which prevent caregivers from offering both modern tumor testing and innovative targeted agents to their patients. We can only overcome these roadblocks by working together in a dedicated team, he adds. To this end, he has great faith in the objectives of the FT3.
“This multi-stakeholder non-profit initiative has a strong focus on patients’ needs and strong backing within industry, this makes for a very good start to create sustainable projects and ultimately lasting value”.
While Dr Westphalen has been working in personalized medicine for a couple of years, he is still very excited about the potential of the FT3 project.
“I hope that we will be able to form a group of dedicated people, growing together with the aim to drive all aspects of precision oncology ultimately improving care for our patients.”
Patients with rare disease often do not have a voice and rely on strong support from family, carers and trusted advocates. On Rare Disease Day 2021, FT3 speaks to advocates for those with a rare disease, who outline the barriers and roadblocks to obtaining a prompt diagnosis and the best possible personalized treatment.
Warnyta Minnaard is the co-founder of Missie Tumor Onbekend, the patient support and advocacy organization for patients with cancer of unknown primary (CUP) in the Netherlands.
Cancer of unknown primary is the fourth most common metastatic cancer in the Netherlands, with about 1,400 Dutch people each year diagnosed with CUP. Missie Tumor Onbekend advocates for a specialized diagnostic and care pathway for CUP patients, better access to innovative diagnostics and (curative/palliative) care. Furthermore, we provide support to patients, share information about CUP, raise awareness and support clinical research to try to find a solution for CUP. About 2.5 years ago my partner Hederik (age 32) suddenly became ill. It all started with a hanging eyelid and we started with a journey in the hospital to try to find out what was wrong. Unfortunately, he passed away in early January 2019 and I became a widow at age 29. Even though he was severely ill, we had no idea he was going to die as we were in the midst of an ongoing diagnostic trajectory that already took seven months. This is more often the case with a CUP diagnosis; you don’t understand that it is a diagnosis to have cancer without knowing the origins.
Patients with CUP are an outlier in the oncology community, as they are metastatic cancer patients but the origin of their disease is unknown and therefore unfortunately their chances towards accessing treatments is still rather limited. You would expect an outlier to be uncommon, but CUP is the eighth most common cancer in the world; because this is such a diverse group of patients, it is challenging to provide a single solution. But it is clear, these patients deserve solutions; it is unbearable to be part of a patient group without evening knowing you are part of the group as your diagnosis is cancer of unknown primary and if nothing is done you will not survive. Furthermore, most cancer therapies are based on the origin of the disease, which is exactly unknown for CUP patients. More than half of CUP patients in the Netherlands pass away in less than two months, so urgency is needed.
I believe the focus should be on improving or changing diagnostics so that there is no longer a strict need to know the localization of the tumor, rather the DNA defects of the tumor cells of the metastases found in the body should become clear. So that treatment can be provided on the basis of molecular patterns and patients get an outlook and a chance towards care instead of staying in a diagnostic trajectory with no end. The developments of personalized diagnostics and treatments are exactly what CUP patients are in dire need of.
Spinal Muscular Atrophy (SMA) is a motor neuron disease. The motor neurons affect the voluntary muscles that are used for activities such as crawling, walking, head and neck control, and swallowing. It is a relatively common “rare disorder”; approximately one in 6,000 babies born are affected, and about 1 in 40 people are genetic carriers.
SMA affects muscles throughout the body, although the proximal muscles (those closest to the trunk of one’s body – i.e. shoulders, hips, and back) are often most severely affected. Weakness in the legs is generally greater than in the arms. Sometimes feeding and swallowing can be affected. Involvement of respiratory muscles (muscles involved in breathing and coughing) can lead to an increased tendency for pneumonia and other lung problems.
Until very recently, there have been no treatments available for SMA patients. At diagnoses, they were simply told to take their children home and love them for as long as they had them. We at Cure SMA Canada offered support for newly diagnosed families, through life and in the event of end of life, we are there as well. We advocated for access to the first treatment that came available for SMA patients and were successful to receive approval in Canada. Unfortunately it wasn’t approved for all patients.
Every stepping stone along the path in the Canadian approval process was faced with barriers and the need for strong advocacy to justify patient access to the only treatment for SMA. The unfortunate loss of life and function during this process was devastating. With a progressive disease such as SMA, every day matters, every day is a loss of function and fear of what the future holds without treatment. We are now in the process of advocating for two new treatments here in Canada, we still have patients not accessing treatment because they fall outside the criteria for these treatments and we are advocating from square one again, justifying and waiting for approval while our patients continue to experience loss of function and experience high anxiety waiting to hear if the federal and provincial governments makes their life and death decisions. When you have a progressive disease, and are experiencing loss of physical abilities, it is even more devastating to know that other jurisdictions are approving treatment. In the meantime, we continue our work, to fight for our patient’s right to live their best life, to justify a life with treatment and hope that we are heard and considered partners in the decisions that will impact quality and quantity of life. Until we have a cure for SMA, the need for new and improved treatments will continue. Clearly involvement in clinical trials is essential for this information to be developed and available for Canadians. We must be participants and not bystanders.
February 28 2021 marks the fourteenth international Rare Disease Day coordinated by EURORDIS. This global event offers patients, families and caregivers the opportunity to raise awareness and share their experiences of living with a rare disease and the arduous journey they often face as they seek diagnosis and treatment for their condition.
It is thought that there are around 7,000 rare or “orphan” diseases, some of which can affect as little as a handful of people worldwide. Advocacy with these small numbers can be difficult, hence Rare Disease Day is a chance to shine a spotlight on all rare diseases as the rare disease community joins together.
The relationship between personalized medicine and rare diseases is a close one – in many circumstances, personalized medicine offered the first opportunity that these patients had of effective treatment for their condition. FT3 has chosen Rare Disease Day 2021 to highlight the struggles that these patients can often face in accessing timely diagnosis and appropriate treatment, and the daily battles that their advocates engage in on their behalf. Here we present some of their stories:
“It is grossly under and mis-diagnosed”
Blaine Penny is the director and co-founder of MitoCanada, a charitable organization formed in 2010 by a group of passionate Canadian parents whose previously healthy children were given a diagnosis of mitochondrial disease. Blaine’s son Evan was one of these.
“There are minimal treatments and no cure for mitochondrial disease. Very few front line clinicians are knowledgeable about mitochondrial disease and there are only a handful of specialists in Canada. It is grossly under and mis-diagnosed, which means people do not know the root cause of the problem, and hence are not getting the best available treatment. MitoCanada estimates that only 20-30% of people with Mito get a diagnosis.
“Current treatments consist of the Mito cocktail, which is a combination of vitamin supplements to help stabilize the mitochondrial function. The Mito Cocktail is the no. 1 prescribed treatment for mito patients but one of the big challenges with this is affordability as only one province in Canada, Ontario, has a provincial Inherited Metabolic Disease Program that covers the cost. Most patients/family are burdened with these costs. Exercise is considered one of the best therapies, but unfortunately many patients (like my son Evan who is a spastic quadriplegic) cannot exercise. Evan is in 11 different clinics, takes 14 different medications and supplements, and requires around the clock nursing care. This is pretty typical of the complex mito patient and puts tremendous pressure on families to coordinate and balance care.
There is some light at the end of the tunnel; NextGen DNA sequencing is proving to be increasingly effective in diagnosing patients. But access to specialists and testing is critical. Earlier diagnosis results in earlier interventions which improves health and quality of life outcomes.”
“Patients are challenged by finding health care providers that have a deep understanding of their rare disease”
Dr Leanne M Ward is Professor of Pediatrics, University of Ottawa and Medical Director, The CHEO Genetic and Metabolic Bone Disease Clinic
I am a pediatric endocrinologist specializing in pediatric bone diseases, of which most are rare diseases. My goal in caring for such patients is to relieve pain and restore mobility. Both surgical and medical management are needed to restore physical functioning in these disorders. But patients are challenged by finding health care providers that have a deep understanding of their rare condition, and gaining access to multidisciplinary care. They are also challenged because the existing treatments for their disease are often symptom-targeted, and do not address the pathobiology of the condition. By getting closer to the actual cause of the disorder and targeting that, we are better able to improve clinical outcomes in a meaningful way.
We need more education of health care professionals, with teams all working together to care for the patient, we need scientists working on the biology of the disease so that therapeutic targets can be identified, and we need clinical trials to be as streamlined and efficient as possible. As it is now, clinical trials are extremely difficult due to the multiple administrative and organizational layers that complicate the already-challenging medical care issues for those patients undergoing trials. I like the idea of “rare disease centers of excellence” that could be beacons of light for patients with rare disorders.
“There are hurdles to overcome at every stage of the BRCA journey”
Abi Jackson is a BRCA breast cancer advocate, based in Ireland. She works closely with the Marie Keating Foundation.
“Breast, bowel and ovarian are some cancers that can run in families, and occur when faulty genes pass down through generations. The lifetime risk for a woman with a BRCA1 mutation is 60-90%. These women additionally have a 40–60% lifetime risk of developing ovarian cancer. Men are often forgotten in discussions about BRCA, but they can carry cancer-causing faulty genes. A man with a BRCA1 mutation may be 3 or 4 times more likely to develop prostate cancer by age 65.
In recent years, largely thanks to the availability of genetic testing and awareness, a growing number of men and women have discovered they have the faulty BRCA gene as a result of pre-symptomatic screening. In my case, screening was offered to me and my siblings when my older sister, then 37 years, was diagnosed with breast cancer. Sadly, this was not the first or last woman in our wider family to receive this diagnosis. Having the knowledge that you are at high risk for breast and ovarian cancer is both a blessing and a burden. Like me, many opt to reduce the risk of developing cancer through surveillance and surgical procedures such as bilateral mastectomy and removal of the ovaries and fallopian tubes. Yet taking this route to protect your health is fraught with challenges at every step of the way.
There are hurdles to overcome at every stage of the BRCA journey. The first is navigating a health service that is not fit for purpose for genetic cancer patients. Getting a referral is not straightforward and often comes about by indirect channels. If you meet the eligibility criteria for genetic screening, you can choose to join a public or private waiting list for genetic counselling. As the clinical genetics service is so poorly resourced in Ireland, this can take many years. If you opt for private genetic counseling, the cost is high. With few exceptions, your care and treatment ends up occurring in silos; breast care clinic, gynaecology clinic, plastic surgery clinic, and psychology services. It is both an art and a science navigating multi-disciplinary care for a person with a faulty BRCA gene.
FT3 is unique in having patients as a fundamental and essential partner, says project member Durhane Wong-Rieger, President & CEO of the Canadian Organization for Rare Disorders
Tell us more about yourself.
Durhane Wong-Rieger – CORD
I am President & CEO of the Canadian Organization for Rare Disorders (CORD). As head of a global alliance of rare disease patient organizations in Canada, we are committed to improving the lives of all Canadian patients and families affected by rare diseases. CORD leads initiatives to change and implement policy, collaborate to improve healthcare infrastructure, services, and access; advocate on behalf of patients for interventions, including innovative medicines, devices, and supportive services and foster research. We also increase the capacity of the patient organizations to take an active role in advocacy and support through a variety of training programs and collaborative projects.
I am a psychologist by training and taught for about 20 years as a university professor before moving to full-time patient advocacy. I have two children born with rare conditions and a spouse with genetic heart disease and Parkinson’s Disease.
What does personalized medicine mean to you?
Personalized medicine is an “umbrella” concept that is inherent to rare diseases, whereby patients receive “targeted” care based on their individual diagnosis (disease, genetic/genomic profile, and lifestyle factors). The “rarer” the condition, the more challenging to get to a diagnosis but also the more critical to get it “precise” so the term “precision” healthcare is probably more applicable. It is more than just medicines and it may not be so much person-specific as targeted. Challenges exist on many levels, from system capacity, healthcare professional readiness, and patient awareness.
Why do you believe this topic is important as a patient advocate?
Raising awareness and educating patients about personalized medicine is essential to accessing what is available and advocating for what could and should be available. Obviously, the patient is key in terms of seeking access and increasing capacity and willingness (that is, resources).
Why is your organization interested in participating in this multi-stakeholder collaboration?
CORD, along with the international rare disease community, has been advancing models and centers for diagnosis, care, and treatment but also the development of innovative therapies (genetically defined and targeted). Our organization supports at the patient level development of patient registries to have patient populations available for clinical trials and to develop natural history studies as well as clinical trial design appropriate for “small, targeted” patient populations. Our organization has also been engaged in helping to define and collect patient outcome evidence, setting up access programs including new financing models for access, and promoting collaboration across all stakeholders so that innovations could be available as soon as possible but also cognizant of needs for sustainability (e.g., managed access, risk-sharing models, amortized financing).
What makes this collaboration unique?
FT3 is the first international collaboration where patients are not just equal partners but indeed an essential, fundamental partner. The patient voice and patient perspective are not just referenced but have primary status in terms of principles but also in decisions on how to proceed.
What are your ultimate expectations from the project?
The most important short-term expectation is that all stakeholders remain committed to the collaboration and the process; we must learn how to work together effectively. Other short-term expectations are the articulation of consensual vision, principles, desired outcomes and from this platform the definition of a working process for the collaborations that translate into meaningful actions. This is all very high level so more concretely, I expect we will identify some existing best practices and transformative initiatives that can be built upon and adapted. That means we need to continue to foster an open sharing environment and avoid competition and “me-first” thinking. I think we are on the right path to get there.
Ralph Riley is a Global Co Dx Market Access Leader with Janssen. As an FT3 member, he believes that the increased adoption of personalized medicine will create value across the entire health ecosystem
Tell us more about yourself.
Ralph Riley – Janssen
I am the Global Co Dx Market Access Leader where I focus on evidence generation activities to help shape policy and payment to enable patient access to testing across all Janssen’s therapeutic areas. The Co Dx Commercial Strategy Group in Janssen supports our pharmaceutical brand initiatives intended to improve patient outcomes by leveraging a variety of precision medicine tools to screen, diagnose, monitor, or select treatments for patients. I have more than 15 years at J&J – including 6 in our device sector in our former clinical diagnostics unit with the remaining time within R&D and Global Commercial Strategy at Janssen.
What does personalized medicine mean to you?
It’s the next generation of healthcare – where the patient gets treated and not just the disease. Personalized medicine leverages technologies to use validated information by a clinician and a patient to jointly make informed and timely choices about potential decisions regarding the patient’s health and well-being. It helps to more precisely answer questions regarding whether a patient is at risk for a disease, which disease a patient may have, how serious their particular disease may be, which treatment may best serve them and how they are doing once on treatment.
Why do you believe this topic is important?
I believe there is no more profound way to create value for the system than to dramatically increase our success in improving health, and prevention plays a major role in more precise treatment of diseases too.
Why is your organization interested in participating in this multi-stakeholder collaboration?
A variety of stakeholders – especially patients – but including providers, industry (pharmaceutical, device, diagnostic, laboratory) and payers are all important. Given the structure of the marketplace, the way to align discussion and demonstration of value for each stakeholder is to leverage a collaboration to listen and work with a common purpose. This means working with trade groups and patient organizations to find common ways to achieve better patient outcomes. These approaches are not new but are invaluable when large, strategic change is in the making.
What makes this collaboration unique?
I think in how it began- and will ultimately finish. With the collaborators directly listening to patients and their desires to give direction to our work. In a way that mirrors what I think personalized medicine means to me…with the patient at the start and finish of our intentions.
What are your ultimate expectations from the project?
Enablement of the dialog between patient and provider to make the best choices for the patient across their journey… with data and evidence to support those decisions…
A recent virtual workshop sought to determine the needs of patients when it comes to personalized or precision medicine. Danielle Barron reports
What is personalized medicine, and what does it mean for the everyday reality of patients?
A uniquely designed workshop at the recent Patient Engagement Open Forum sought to answer these questions by seeking to understand the landscape of information and support needs of the patient community (and others) in order to make informed decisions around personalized (or precision) medicine at various points in time.
Hosted by PARADIGM, PFMD and EUPATI, the Patient Engagement Open forum is a series of virtual events where a broad range of stakeholders aim to work together to turn patient engagement into reality. Although it migrated online this year, a large and eager audience still participated in each of the interactive and dynamic workshops.
“From diagnosis to treatment and beyond: personalized medicine – what’s in it for patients and understanding patient needs to make it a reality?” was the workshop led by the “From Testing to Treatment Program” (FT3). The program aims to accelerate the benefits of Personalized Medicine and Precision Medicine (PM) by generating better evidence, creating awareness and building the conditions for better access to targeted medicine in oncology and beyond.
FT3 is a global, open and collaborative multistakeholder program that aims to build synergies and accelerate pragmatic efforts to make PM an accessible reality for all those who could benefit from it, starting with oncology and testing.
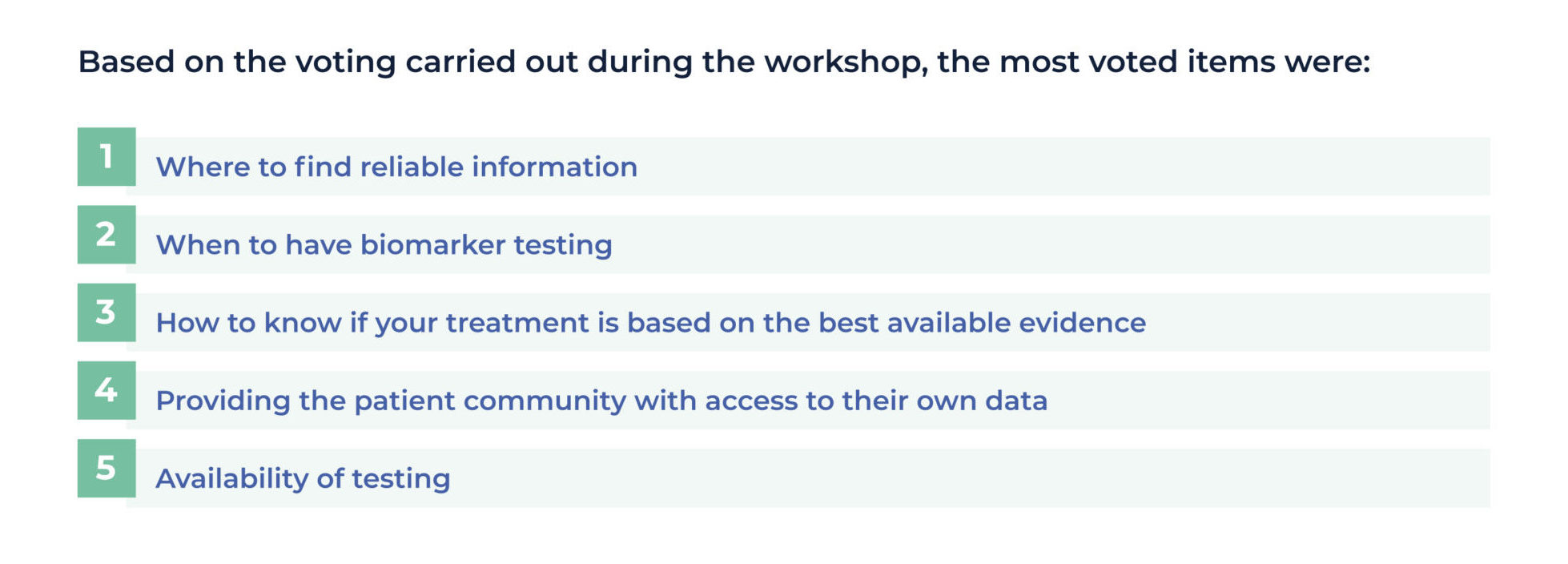
During this PE Open Forum workshop, attendees participated in an interactive exercise aimed at understanding the landscape of information and support needs of the patient community (and others) in order to make informed decisions around PM at various points in time. The insights gathered will inform the co-creating of PM support and information materials for the patient community, supplementing existing resources and tailoring the content to best address the unmet needs of patients.
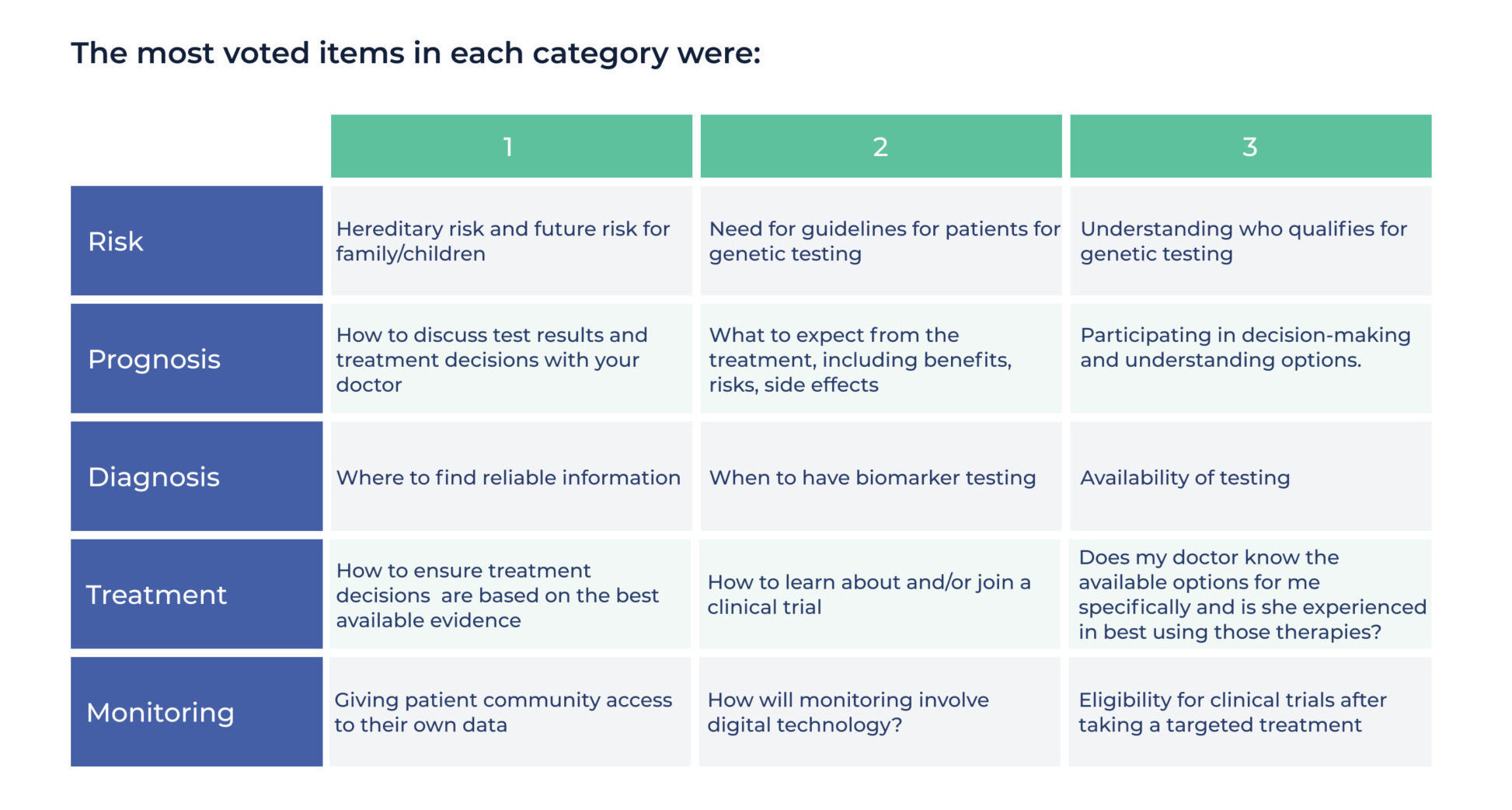
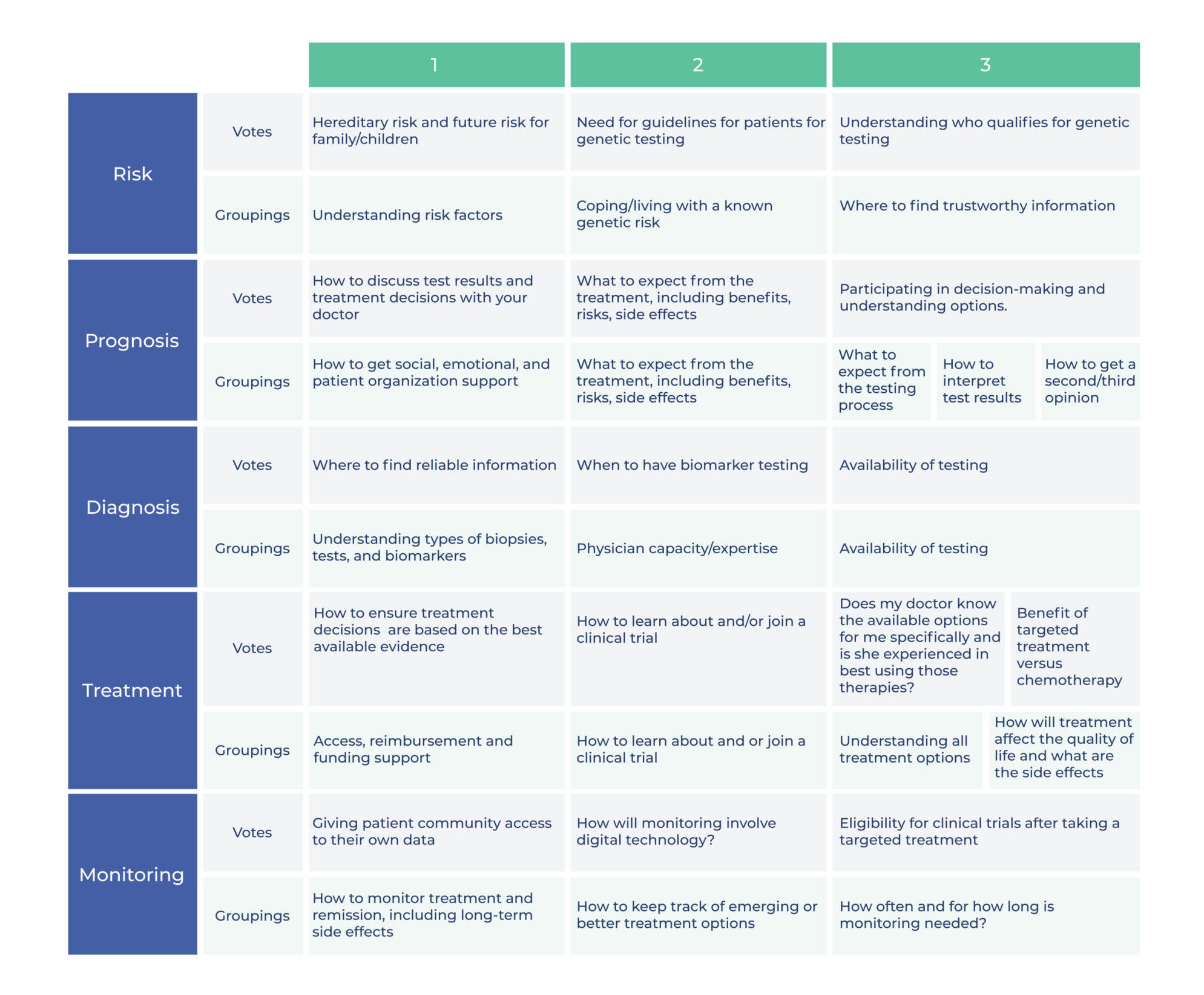
Each patient experience is different, but the workshop aimed to highlight distinct ‘moments’ that are relevant from a patient perspective in terms of personalized and precision medicine. These were: Risk; Prognosis; Diagnosis; Treatment; and Monitoring. Patients were asked to identify their needs as they related to each of these distinct aspects of their experience so that a picture could be painted of changing requirements at these different and discrete moments.
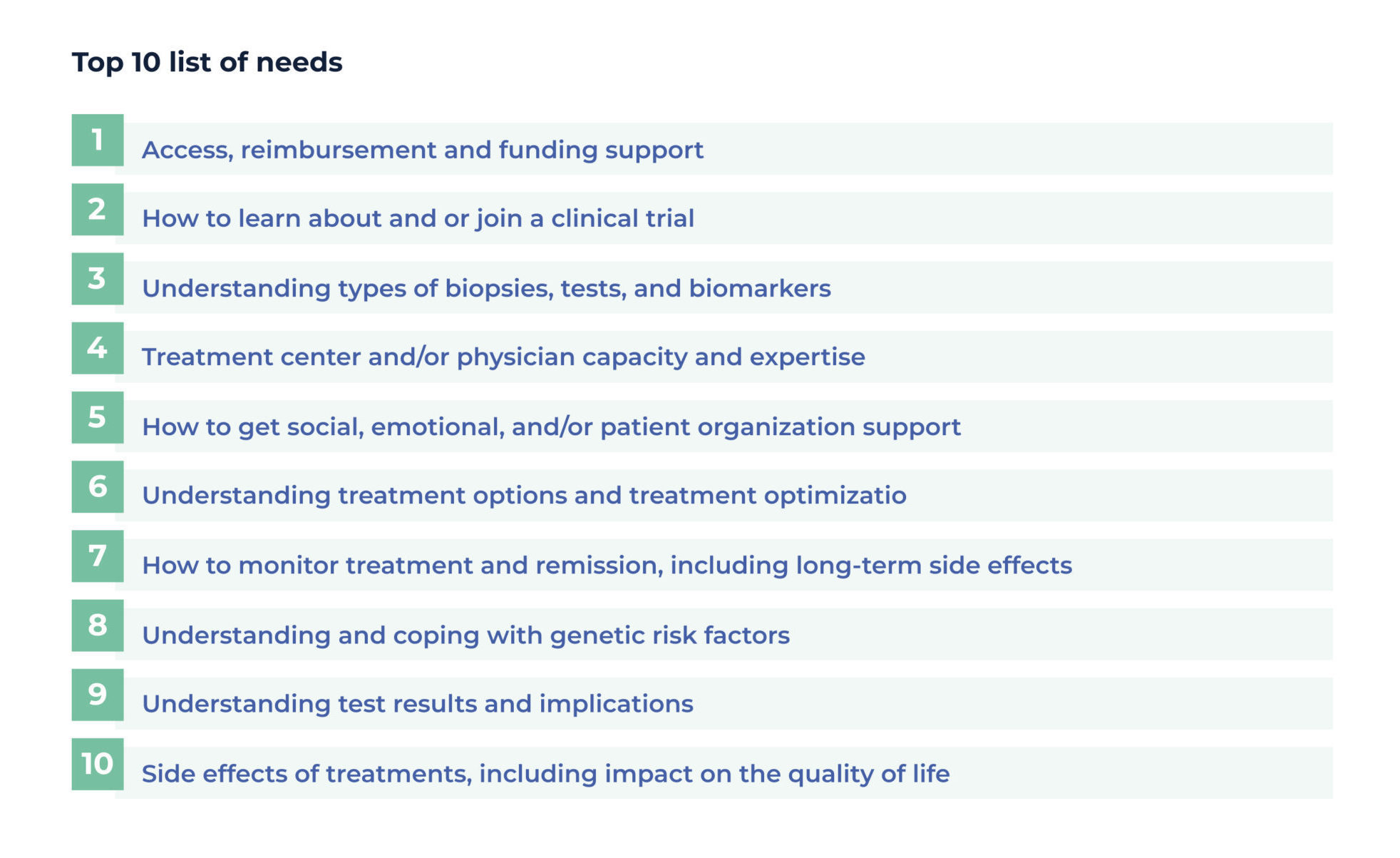
In total, a staggering 220 support and information needs were identified during the workshop. Grouping these and assimilating similar suggestions led to a “top 10” list of needs, which helped to paint a picture of the myriad questions patients understandably have about all aspects of their diagnosis, prognosis, treatment and outcomes. What emerged was that patients are missing or don’t know where to find information crucial to each aspect of their patient experience, from initial diagnosis to treatment to living with the condition.
Although these are simply a sample of the hundreds if needs identified during the workshop, they were those that were shared by the largest number of patients who participated. These insights will now be considered as the FT3 begins its co-creation initiative with patients.
Leslie Manot was a patient representative who spoke powerfully about her personal experience with rare lung cancer during the session. She praised the “brainstorming” format utilized within the workshop, saying it compared favorably to other similar webinars or web conferences.
“The format was very clear and well prepared,” said Manot. “The instructions were easy to understand and the results quickly readable.” She added that this event was hugely important, as it was a great opportunity for patients to pool their knowledge and strengths in order to improve their care at an international level.
Manot noted that it was a learning curve for patients too, helping them to understand that the struggles or difficulties they may face, other patients around the world face them too. “The surprise for me was to understand that most of the participants have the same issue as in France for test availability and drug market access.” She added she hopes the results will form the basis for discussions with the relevant authorities on the wide disparities in innovation access.
Why is it so important to capture patient insights? Manot said: “The patients are becoming experts in their disease, as due to internet utilization they have access to medical information, and they can share their experiences with other patients. Some of them even have a diploma to show they are a ‘patient-expert’. The professionals have knowledge but patients have experience.”